CURRENT AFFAIRS – 07/06/2024
- CURRENT AFFAIRS – 07/06/2024
- NHRC seeks report on Nata Pratha practice / NHRC ने नाता प्रथा पर रिपोर्ट मांगी
- 65.79% turnout in 2024 Lok Sabha election, says EC / चुनाव आयोग ने कहा कि 2024 के लोकसभा चुनाव में 65.79% मतदान होगा
- ‘India must spend up to 5 bn for RE goal’ / ‘भारत को RE लक्ष्य के लिए 385 बिलियन डॉलर तक खर्च करना होगा’
- Regulator SEBI expands promoter definition for IPO-bound companies / नियामक सेबी ने आईपीओ-बाउंड कंपनियों के लिए प्रमोटर परिभाषा का विस्तार किया
- Russia defends OPEC+ oil pact, says may tweak if needed / रूस ने ओपेक+ तेल समझौते का बचाव किया, कहा कि ज़रूरत पड़ने पर इसमें बदलाव किया जा सकता है
- The roads to India’s redemocratisation, the challenges / भारत के पुनर्लोकतंत्रीकरण की राहें, चुनौतियाँ
- Australia and Oceania [Mapping] / ऑस्ट्रेलिया और ओशिनिया [मानचित्र]
CURRENT AFFAIRS – 07/06/2024
NHRC seeks report on Nata Pratha practice / NHRC ने नाता प्रथा पर रिपोर्ट मांगी
(General Studies- Paper I)
Source : The Hindu
Nata Pratha
- Nata Pratha is a harmful traditional practice prevalent in certain communities in states like Rajasthan, Madhya Pradesh, Uttar Pradesh, and Gujarat.
- It involves the selling of girls, either on stamp paper or through informal means, under the pretext of illegal or child marriage.
- Often, these transactions are orchestrated by the girls’ own families.
- The practice results in severe violations of human rights and contributes to the perpetuation of gender inequality and exploitation.
- Girls subjected to Nata Pratha face physical, emotional, and psychological trauma, as they are essentially treated as commodities.
- The National Human Rights Commission (NHRC) has deemed the practice immoral and called for its immediate eradication and abolition.
- It has directed concerned states to submit reports on measures taken or proposed to address Nata Pratha within eight weeks.
- The NHRC recommends prosecuting individuals involved in forcing women into Nata Pratha under laws related to human trafficking to combat this egregious violation of human dignity.
NHRC ने नाता प्रथा पर रिपोर्ट मांगी
नाता प्रथा
- नाता प्रथा राजस्थान, मध्य प्रदेश, उत्तर प्रदेश और गुजरात जैसे राज्यों में कुछ समुदायों में प्रचलित एक हानिकारक पारंपरिक प्रथा है।
- इसमें अवैध या बाल विवाह के बहाने स्टाम्प पेपर पर या अनौपचारिक माध्यमों से लड़कियों को बेचा जाता है।
- अक्सर, ये लेन-देन लड़कियों के अपने परिवारों द्वारा ही किए जाते हैं।
- इस प्रथा के परिणामस्वरूप मानवाधिकारों का गंभीर उल्लंघन होता है और लैंगिक असमानता और शोषण को बढ़ावा मिलता है।
- नाता प्रथा की शिकार लड़कियों को शारीरिक, भावनात्मक और मनोवैज्ञानिक आघात का सामना करना पड़ता है, क्योंकि उनके साथ अनिवार्य रूप से वस्तुओं जैसा व्यवहार किया जाता है।
- राष्ट्रीय मानवाधिकार आयोग (NHRC) ने इस प्रथा को अनैतिक माना है और इसके तत्काल उन्मूलन और उन्मूलन का आह्वान किया है।
- इसने संबंधित राज्यों को नाता प्रथा से निपटने के लिए उठाए गए या प्रस्तावित उपायों पर आठ सप्ताह के भीतर रिपोर्ट प्रस्तुत करने का निर्देश दिया है।
- NHRC ने मानव गरिमा के इस गंभीर उल्लंघन से निपटने के लिए मानव तस्करी से संबंधित कानूनों के तहत महिलाओं को नाता प्रथा में धकेलने में शामिल व्यक्तियों पर मुकदमा चलाने की सिफारिश की है।
65.79% turnout in 2024 Lok Sabha election, says EC / चुनाव आयोग ने कहा कि 2024 के लोकसभा चुनाव में 65.79% मतदान होगा
(General Studies- Paper II)
Source : The Hindu
Highlights
- The recently concluded 2024 Lok Sabha election had a turnout of 65.79%, slightly lower than 2019’s 67.4%.
- Chief Election Commissioner Rajiv Kumar stated that approximately 64.2 crore voters participated.
- Lakshadweep recorded the highest turnout at 84%, followed by Assam at 81%, while Bihar had the lowest at 56.19%.
- Uttar Pradesh and Mizoram also had low turnouts, with 56.92% and 56.87% respectively.
- The final figures may change pending inclusion of postal ballots.
- The overall voter turnout for the seventh phase was 63.88%.
- The Election Commission submitted the list of elected MPs to President Droupadi Murmu as per the Representation of People’s Act.
- Narendra Modi, after the BJP-led NDA’s majority win, is set to take oath for a third consecutive term on June 9.
चुनाव आयोग ने कहा कि 2024 के लोकसभा चुनाव में 65.79% मतदान होगा
मुख्य बातें
- हाल ही में संपन्न 2024 के लोकसभा चुनाव में 79% मतदान हुआ, जो 2019 के 67.4% से थोड़ा कम है।
- मुख्य चुनाव आयुक्त राजीव कुमार ने कहा कि लगभग 2 करोड़ मतदाताओं ने भाग लिया।
- लक्षद्वीप में सबसे अधिक 84% मतदान हुआ, उसके बाद असम में 81% मतदान हुआ, जबकि बिहार में सबसे कम 19% मतदान हुआ।
- उत्तर प्रदेश और मिजोरम में भी कम मतदान हुआ, जहाँ क्रमशः 92% और 56.87% मतदान हुआ।
- पोस्टल बैलेट को शामिल किए जाने के बाद अंतिम आँकड़े बदल सकते हैं।
- सातवें चरण के लिए कुल मतदान 88% रहा।
- चुनाव आयोग ने जनप्रतिनिधित्व अधिनियम के अनुसार राष्ट्रपति द्रौपदी मुर्मू को निर्वाचित सांसदों की सूची सौंपी।
- भाजपा के नेतृत्व वाली एनडीए की बहुमत की जीत के बाद नरेंद्र मोदी 9 जून को लगातार तीसरी बार शपथ लेने वाले हैं।
‘India must spend up to 5 bn for RE goal’ / ‘भारत को RE लक्ष्य के लिए 385 बिलियन डॉलर तक खर्च करना होगा’
(General Studies- Paper III)
Source : The Hindu
- India will have to invest as much as $385 billion to meet its target of 500 gigawatts (GW) of renewable energy (RE) by 2030, but coal will remain a key source of electricity generation for the next decade, Moody’s Ratings said.
- India, a major greenhouse gas emitter, said it aims to ramp up non-fossil fuel capacity set by 50 GW each year to help meet 500 GW target. It missed its target of 175 GW by 2022.
- Moody’s, however, estimates an annual capacity addition of about 44 GW will help achieve the goal.
- For that, India will have to spend $190 billion to $215 billion on capacity over the next six to seven years and another $150 billion to $170 billion for transmission and distribution, the credit ratings agency estimates.
- India’s strong policy support boosted the RE share to about 43% in its power capacity mix in fiscal 2023-24, attracting private investments.
‘भारत को RE लक्ष्य के लिए 385 बिलियन डॉलर तक खर्च करना होगा’
- मूडीज रेटिंग्स ने कहा कि भारत को 2030 तक 500 गीगावाट (GW) अक्षय ऊर्जा (RE) के अपने लक्ष्य को पूरा करने के लिए 385 बिलियन डॉलर तक का निवेश करना होगा, लेकिन कोयला अगले दशक तक बिजली उत्पादन का प्रमुख स्रोत बना रहेगा।
- भारत, एक प्रमुख ग्रीनहाउस गैस उत्सर्जक, ने कहा कि इसका लक्ष्य 50 गीगावाट प्रति वर्ष निर्धारित गैर-जीवाश्म ईंधन क्षमता को बढ़ाना है ताकि 500 गीगावाट लक्ष्य को पूरा करने में मदद मिल सके। यह 2022 तक 175 गीगावाट के अपने लक्ष्य से चूक गया।
- हालांकि, मूडीज का अनुमान है कि लगभग 44 गीगावाट की वार्षिक क्षमता वृद्धि लक्ष्य को प्राप्त करने में मदद करेगी।
- इसके लिए, भारत को अगले छह से सात वर्षों में क्षमता पर 190 बिलियन से 215 बिलियन डॉलर और ट्रांसमिशन और वितरण के लिए 150 बिलियन से 170 बिलियन डॉलर खर्च करने होंगे, क्रेडिट रेटिंग एजेंसी का अनुमान है।
- भारत के मजबूत नीति समर्थन ने वित्त वर्ष 2023-24 में अपने बिजली क्षमता मिश्रण में RE हिस्सेदारी को लगभग 43% तक बढ़ा दिया, जिससे निजी निवेश आकर्षित हुए।
Regulator SEBI expands promoter definition for IPO-bound companies / नियामक सेबी ने आईपीओ-बाउंड कंपनियों के लिए प्रमोटर परिभाषा का विस्तार किया
(General Studies- Paper III)
Source : The Hindu
The stock exchanges have broadened the definition of promoters for companies going public, now including founders collectively holding 10% or more and their immediate relatives if they are on the board or key managerial personnel.
- Old Definition:
- Under current SEBI regulations, a promoter is someone who controls the company’s affairs, appoints the majority of directors, or is named as such in an offer document.
- Founders holding 25% were considered promoters due to their negative control and power to block special resolutions.
- New Definition:
- SEBI now insists that founders holding 10% or more classify themselves as promoters for IPO-bound companies.
- The new guidelines extend to founders collectively holding 10% if they are key managerial personnel (KMP) or directors.
- Immediate relatives of promoters will also be deemed promoters if they hold 10% or more in the company, directly or indirectly.
- This expansion of the definition encompasses relatives who are not involved in management or board roles but hold significant shares, significantly broadening the promoter group’s scope.
नियामक सेबी ने आईपीओ-बाउंड कंपनियों के लिए प्रमोटर परिभाषा का विस्तार किया
स्टॉक एक्सचेंजों ने सार्वजनिक होने वाली कंपनियों के लिए प्रवर्तकों की परिभाषा को व्यापक बना दिया है, अब इसमें सामूहिक रूप से 10% या उससे अधिक हिस्सेदारी रखने वाले संस्थापक और उनके निकटतम रिश्तेदार (यदि वे बोर्ड या प्रमुख प्रबंधकीय कर्मचारी हैं) भी शामिल हैं।
पुरानी परिभाषा:
- वर्तमान सेबी नियमों के तहत, प्रमोटर वह व्यक्ति होता है जो कंपनी के मामलों को नियंत्रित करता है, अधिकांश निदेशकों को नियुक्त करता है, या किसी प्रस्ताव दस्तावेज़ में इस तरह नामित होता है।
- 25% हिस्सेदारी रखने वाले संस्थापकों को उनके नकारात्मक नियंत्रण और विशेष प्रस्तावों को रोकने की शक्ति के कारण प्रमोटर माना जाता था।
नई परिभाषा:
- सेबी अब जोर देता है कि 10% या उससे अधिक हिस्सेदारी रखने वाले संस्थापक खुद को आईपीओ-बाउंड कंपनियों के प्रमोटर के रूप में वर्गीकृत करते हैं।
- नए दिशानिर्देश सामूहिक रूप से 10% हिस्सेदारी रखने वाले संस्थापकों पर लागू होते हैं, यदि वे प्रमुख प्रबंधकीय कर्मी (केएमपी) या निदेशक हैं।
- प्रमोटरों के तत्काल रिश्तेदार भी प्रमोटर माने जाएंगे, यदि वे प्रत्यक्ष या अप्रत्यक्ष रूप से कंपनी में 10% या उससे अधिक हिस्सेदारी रखते हैं।
- परिभाषा के इस विस्तार में ऐसे रिश्तेदार शामिल हैं जो प्रबंधन या बोर्ड की भूमिकाओं में शामिल नहीं हैं, लेकिन महत्वपूर्ण शेयर रखते हैं, जिससे प्रमोटर समूह का दायरा काफी बढ़ गया है।
Russia defends OPEC+ oil pact, says may tweak if needed / रूस ने ओपेक+ तेल समझौते का बचाव किया, कहा कि ज़रूरत पड़ने पर इसमें बदलाव किया जा सकता है
(General Studies- Paper II)
Source : The Hindu
OPEC+
- It is a group of oil-exporting countries which meets regularly to decide how much crude oil to sell on the world market.
- Origin: These nations came to an accord towards the end of 2016 “to institutionalize a framework for cooperation between OPEC and non-OPEC producing countries on a regular and sustainable basis.”
- These nations aim to work together on adjusting crude oil production to bring stability to the oil market.
- OPEC+ controls about 40% of global oil supplies and more than 80% of proven oil reserves.
- At the core of this group are the members of OPEC (the Organization of the Oil Exporting Countries), which are mainly Middle Eastern and African countries.
- Members: It comprises OPEC countries plus Azerbaijan, Bahrain, Brunei, Kazakhstan, Russia, Mexico, Malaysia, South Sudan, Sudan, and Oman.
Highlights of the news
OPEC+ is balancing oil supply and demand by extending output cuts into 2025, with some members phasing out voluntary cuts gradually. Brent crude prices dropped below $80 per barrel, a critical level for many members’ budgets.
- OPEC+ is extending most of its oil output cuts into 2025, aimed at balancing oil supply and demand and providing market stability.
- Russian Deputy Prime Minister Alexander Novak emphasized the group’s readiness to adjust the agreement if necessary to support the market.
- Following the extension announcement, Brent crude oil prices fell below $80 per barrel, a key price level for many OPEC+ members to balance their budgets.
- The Organization of the Petroleum Exporting Countries (OPEC) and its allies, including Russia, have been implementing deep output cuts since late 2022.
- Currently, OPEC+ members are cutting production by 5.86 million barrels per day (bpd), approximately 5.7% of global demand.
- In addition to these cuts, some members, including Russia, agreed to phase out voluntary cuts of 2.2 million bpd from October 2023 to September 2025.
- Alexander Novak stated that Russia is working on establishing its oil production capacity by autumn 2025.
- OPEC+ aims to agree on oil production capacity for member countries by the end of 2024, addressing a historically contentious issue since each nation’s output target is based on its notional capacity.
रूस ने ओपेक+ तेल समझौते का बचाव किया, कहा कि ज़रूरत पड़ने पर इसमें बदलाव किया जा सकता है
OPEC+
- यह तेल निर्यातक देशों का एक समूह है जो विश्व बाजार में कितना कच्चा तेल बेचना है, यह तय करने के लिए नियमित रूप से मिलते हैं।
- उत्पत्ति: ये राष्ट्र 2016 के अंत में “ओपेक और गैर-ओपेक उत्पादक देशों के बीच नियमित और टिकाऊ आधार पर सहयोग के लिए एक ढांचे को संस्थागत बनाने” के लिए एक समझौते पर पहुंचे।
- ये राष्ट्र तेल बाजार में स्थिरता लाने के लिए कच्चे तेल के उत्पादन को समायोजित करने पर मिलकर काम करने का लक्ष्य रखते हैं।
- ओपेक+ वैश्विक तेल आपूर्ति का लगभग 40% और सिद्ध तेल भंडार का 80% से अधिक नियंत्रित करता है।
- इस समूह के मूल में ओपेक (तेल निर्यातक देशों का संगठन) के सदस्य हैं, जो मुख्य रूप से मध्य पूर्वी और अफ्रीकी देश हैं।
- सदस्य: इसमें ओपेक देशों के अलावा अज़रबैजान, बहरीन, ब्रुनेई, कजाकिस्तान, रूस, मैक्सिको, मलेशिया, दक्षिण सूडान, सूडान और ओमान शामिल हैं।
समाचार के मुख्य अंश
- ओपेक+ 2025 तक उत्पादन में कटौती को बढ़ाकर तेल की आपूर्ति और मांग को संतुलित कर रहा है, कुछ सदस्य धीरे-धीरे स्वैच्छिक कटौती को समाप्त कर रहे हैं। ब्रेंट क्रूड की कीमतें 80 डॉलर प्रति बैरल से नीचे गिर गईं, जो कई सदस्यों के बजट के लिए एक महत्वपूर्ण स्तर है।
- ओपेक+ अपने अधिकांश तेल उत्पादन में कटौती को 2025 तक बढ़ा रहा है, जिसका उद्देश्य तेल की आपूर्ति और मांग को संतुलित करना और बाजार में स्थिरता प्रदान करना है।
- रूसी उप प्रधान मंत्री अलेक्जेंडर नोवाक ने बाजार का समर्थन करने के लिए यदि आवश्यक हो तो समझौते को समायोजित करने के लिए समूह की तत्परता पर जोर दिया।
- विस्तार की घोषणा के बाद, ब्रेंट कच्चे तेल की कीमतें 80 डॉलर प्रति बैरल से नीचे गिर गईं, जो कई ओपेक+ सदस्यों के लिए अपने बजट को संतुलित करने के लिए एक महत्वपूर्ण मूल्य स्तर है।
- पेट्रोलियम निर्यातक देशों का संगठन (ओपेक) और रूस सहित इसके सहयोगी 2022 के अंत से भारी उत्पादन कटौती को लागू कर रहे हैं।
- वर्तमान में, ओपेक+ सदस्य 86 मिलियन बैरल प्रति दिन (बीपीडी) उत्पादन में कटौती कर रहे हैं, जो वैश्विक मांग का लगभग 5.7% है।
- इन कटौतियों के अलावा, रूस सहित कुछ सदस्य अक्टूबर 2023 से सितंबर 2025 तक 2 मिलियन बीपीडी की स्वैच्छिक कटौती को चरणबद्ध तरीके से समाप्त करने पर सहमत हुए।
- अलेक्जेंडर नोवाक ने कहा कि रूस 2025 की शरद ऋतु तक अपनी तेल उत्पादन क्षमता स्थापित करने पर काम कर रहा है।
- ओपेक+ का लक्ष्य 2024 के अंत तक सदस्य देशों के लिए तेल उत्पादन क्षमता पर सहमत होना है, जो ऐतिहासिक रूप से विवादास्पद मुद्दे को संबोधित करता है क्योंकि प्रत्येक देश का उत्पादन लक्ष्य उसकी काल्पनिक क्षमता पर आधारित है।
The roads to India’s redemocratisation, the challenges / भारत के पुनर्लोकतंत्रीकरण की राहें, चुनौतियाँ
(General Studies- Paper II)
Source : The Hindu
Context
- The article discusses systemic failures in health-care regulations following a tragic fire incident in a New Delhi neonatal care nursing home.
- It highlights challenges in implementing unrealistic regulations, unfair practices in scrutinising private facilities, and the need for reforms to promote affordable and accessible health care.
Health care regulations
- The subject of regulation has always been of interest to health programme managers but, arguably, is one of the weakest points in India’s health-care system.
- It is not as if there are not enough health regulations in Indian States. Rather, it is a problem of excess.
- Some States have over 50 approvals under multiple regulations, which need to be followed and complied with by every health-care facility.
- The other challenge is unrealistic health-care quality standards. Governments at every level in India — national and States — are known to draft policies which are near perfect.
- One such case is the Clinical Establishments (Registration and Regulation) Act, 2010, enacted 14 years ago, but not adopted by States.
- This is because State governments, in discussions with stakeholders, have realised that many provisions in the Act are impossible to implement.
- Another example is the Indian Public Health Standards, or IPHS, drafted by the government for its own health-care facilities and proposed as essential in order to deliver quality health services.
- The IPHS were first released in 2007 and have been revised twice since then.
- Yet, in 17 years of existence, only 15% to 18% of government primary health-care facilities in India meet the government’s own standards.
- Clearly, in the efforts to be aspirational, health-care regulations and standards in India have drifted towards unrealistic standards, and are difficult to implement.
India has a mixed health-care system
- There is a binary perception that when it comes to adhering to the rules, the government health sector always does better, and that the private sector always violates them.
- The fact is that India has a mixed health-care system, where private health-care facilities and providers deliver nearly 70% of outpatient and 50% of hospital-based services.
- In most States such as Maharashtra or Kerala, the health indicators are better not because these States have outstanding government facilities but because the facilities and clinics in the private sector are fulfilling the health needs of the people.
- Clearly, for effective regulation and adherence, the stakeholder should not feel they are being targeted.
- In health-care regulation, in the current scheme of things, the burden of responsibility is more on providers and facility owners.
- Most private nursing homes and clinics have often flagged the issue of approvals being delayed by the authorities for months even when these facilities apply for renewal well in advance.
- The sluggish approval process is a main concern as far as facility owners are concerned.
Affordable care is one need
- The private sector is also not a homogenous entity as there is everything from single doctor clinics, small nursing homes and medium-sized hospitals to large corporate hospitals.
- Single doctor clinics and small nursing homes are often the first point of contact for access and utilisation of health services in India by middle-income and low-income populations, and are the real lifeline of health services.
- They deliver a large share of health services at a fraction of cost of that of the big corporate hospitals.
- The single doctor clinics and nursing homes play a key role in health service delivery in India and make services accessible and affordable.
- Clearly, there needs to be supportive and facilitatory regulations to serve the public purpose of keeping health-care costs low and affordable.
Suggestions
- First, ensuring quality of health services is essential and the joint responsibility of all stakeholders.
- Second, in regulatory aspects, what is possible for large corporate hospitals may not be feasible for smaller clinics and nursing homes, without escalated cost.
- Third, representatives of doctors’ associations and the types of facilities for which regulations are being formed as well as community members should be involved in the process of the formulation of such regulation.
- Fourth, political loose talk and sensational media headlines might worsen the mistrust of the common man about doctors and nursing homes and may result in increased violence against health-care providers.
- Fifth, and most importantly, India needs to promote single doctor clinics apart from smaller health-care facilities, and nursing homes.
Conclusion
- India’s health-care system is already becoming skewed towards admission based in-patient services. It needs to promote providers and facilities that deliver out-patient care at lower costs.
- This would contribute to the goal of the National Health Policy, 2017 — to deliver health services that should be people-centric, accessible, available, affordable, and have quality..
Healthcare Regulation in India
Challenges in Healthcare Regulation in India: Fragmented Regulatory Framework
- Lack of a unified regulatory framework results in overlapping jurisdictions and inconsistencies.
- Quality Control: Ensuring quality standards across public and private healthcare providers remains a challenge.
- Access Disparities: Rural-urban divide and socioeconomic disparities affect equitable access to healthcare services.
- Medical Education: Regulation of medical education and accreditation of healthcare institutions require improvement to maintain quality standards.
- Corruption and Oversight: Lack of effective monitoring and oversight mechanisms leads to corruption and malpractices in the healthcare sector.
Way Forward
- Unified Regulatory Body: Establish a unified regulatory body to streamline healthcare regulation and ensure consistency.
- Enhanced Oversight: Strengthen monitoring and enforcement mechanisms to prevent malpractices and ensure compliance with regulations.
- Standardisation of Quality: Implement standardised quality control measures across healthcare facilities to ensure uniform standards of care.
- Investment in Rural Healthcare: Increase investment in rural healthcare infrastructure and services to address access disparities.
- Capacity Building: Invest in training and capacity building for healthcare professionals to enhance service delivery and quality of care.
भारत के पुनर्लोकतंत्रीकरण की राहें, चुनौतियाँ
प्रसंग:
- लेख में नई दिल्ली के नवजात शिशु देखभाल नर्सिंग होम में आग लगने की दुखद घटना के बाद स्वास्थ्य देखभाल विनियमन में प्रणालीगत विफलताओं पर चर्चा की गई है।
- यह अवास्तविक विनियमनों को लागू करने में चुनौतियों, निजी सुविधाओं की जांच में अनुचित प्रथाओं और सस्ती और सुलभ स्वास्थ्य देखभाल को बढ़ावा देने के लिए सुधारों की आवश्यकता पर प्रकाश डालता है।
स्वास्थ्य देखभाल विनियमन:
- विनियमन का विषय हमेशा स्वास्थ्य कार्यक्रम प्रबंधकों के लिए रुचि का विषय रहा है, लेकिन यकीनन यह भारत की स्वास्थ्य देखभाल प्रणाली में सबसे कमजोर बिंदुओं में से एक है।
- ऐसा नहीं है कि भारतीय राज्यों में पर्याप्त स्वास्थ्य विनियमन नहीं हैं।
- बल्कि, यह अधिकता की समस्या है। कुछ राज्यों में कई विनियमनों के तहत 50 से अधिक स्वीकृतियाँ हैं, जिनका पालन और अनुपालन हर स्वास्थ्य देखभाल सुविधा द्वारा किया जाना चाहिए।
- दूसरी चुनौती अवास्तविक स्वास्थ्य देखभाल गुणवत्ता मानक हैं। भारत में हर स्तर पर सरकारें – राष्ट्रीय और राज्य – ऐसी नीतियों का मसौदा तैयार करने के लिए जानी जाती हैं जो लगभग परिपूर्ण होती हैं।
- ऐसा ही एक मामला नैदानिक प्रतिष्ठान (पंजीकरण और विनियमन) अधिनियम, 2010 है, जिसे 14 साल पहले अधिनियमित किया गया था, लेकिन राज्यों द्वारा अपनाया नहीं गया।
- ऐसा इसलिए है क्योंकि राज्य सरकारों ने हितधारकों के साथ चर्चा में महसूस किया है कि अधिनियम में कई प्रावधानों को लागू करना असंभव है।
- एक और उदाहरण भारतीय सार्वजनिक स्वास्थ्य मानक या आईपीएचएस है, जिसे सरकार ने अपनी स्वास्थ्य देखभाल सुविधाओं के लिए तैयार किया है और गुणवत्तापूर्ण स्वास्थ्य सेवाएं प्रदान करने के लिए इसे आवश्यक बताया है।
- आईपीएचएस को पहली बार 2007 में जारी किया गया था और तब से दो बार संशोधित किया गया है।
- फिर भी, 17 वर्षों के अस्तित्व में, भारत में केवल 15% से 18% सरकारी प्राथमिक स्वास्थ्य देखभाल सुविधाएँ ही सरकार के अपने मानकों को पूरा करती हैं।
- स्पष्ट रूप से, आकांक्षात्मक होने के प्रयासों में, भारत में स्वास्थ्य देखभाल नियम और मानक अवास्तविक मानकों की ओर बढ़ गए हैं, और उन्हें लागू करना मुश्किल है।
भारत में एक मिश्रित स्वास्थ्य देखभाल प्रणाली है:
- एक द्विआधारी धारणा है कि जब नियमों का पालन करने की बात आती है, तो सरकारी स्वास्थ्य क्षेत्र हमेशा बेहतर प्रदर्शन करता है, और निजी क्षेत्र हमेशा उनका उल्लंघन करता है।
- वास्तविकता यह है कि भारत में एक मिश्रित स्वास्थ्य देखभाल प्रणाली है, जहाँ निजी स्वास्थ्य देखभाल सुविधाएँ और प्रदाता लगभग 70% आउटपेशेंट और 50% अस्पताल-आधारित सेवाएँ प्रदान करते हैं।
- महाराष्ट्र या केरल जैसे अधिकांश राज्यों में स्वास्थ्य संकेतक बेहतर हैं, न कि इसलिए कि इन राज्यों में उत्कृष्ट सरकारी सुविधाएँ हैं, बल्कि इसलिए कि निजी क्षेत्र की सुविधाएँ और क्लीनिक लोगों की स्वास्थ्य आवश्यकताओं को पूरा कर रहे हैं।
- स्पष्ट रूप से, प्रभावी विनियमन और अनुपालन के लिए, हितधारकों को यह महसूस नहीं होना चाहिए कि उन्हें निशाना बनाया जा रहा है।
- स्वास्थ्य सेवा विनियमन में, वर्तमान योजना के अनुसार, जिम्मेदारी का बोझ प्रदाताओं और सुविधा मालिकों पर अधिक है।
- अधिकांश निजी नर्सिंग होम और क्लीनिक अक्सर अधिकारियों द्वारा महीनों तक अनुमोदन में देरी के मुद्दे को उठाते रहे हैं, भले ही ये सुविधाएँ पहले से ही नवीनीकरण के लिए आवेदन करती हों।
- सुविधा मालिकों के लिए सुस्त अनुमोदन प्रक्रिया एक मुख्य चिंता का विषय है।
किफायती देखभाल एक ज़रूरत है
- निजी क्षेत्र भी एक समरूप इकाई नहीं है क्योंकि इसमें एकल डॉक्टर क्लीनिक, छोटे नर्सिंग होम और मध्यम आकार के अस्पतालों से लेकर बड़े कॉर्पोरेट अस्पताल तक सब कुछ है।
- अकेले डॉक्टर क्लीनिक और छोटे नर्सिंग होम अक्सर भारत में मध्यम आय और निम्न आय वाली आबादी द्वारा स्वास्थ्य सेवाओं की पहुँच और उपयोग के लिए संपर्क का पहला बिंदु होते हैं, और स्वास्थ्य सेवाओं की वास्तविक जीवन रेखा हैं।
- वे बड़े कॉरपोरेट अस्पतालों की तुलना में बहुत कम लागत पर स्वास्थ्य सेवाओं का एक बड़ा हिस्सा प्रदान करते हैं।
- एकल डॉक्टर क्लीनिक और नर्सिंग होम भारत में स्वास्थ्य सेवा वितरण में महत्वपूर्ण भूमिका निभाते हैं और सेवाओं को सुलभ और किफायती बनाते हैं।
- स्पष्ट रूप से, स्वास्थ्य सेवा लागत को कम और किफायती रखने के सार्वजनिक उद्देश्य को पूरा करने के लिए सहायक और सुविधाजनक विनियमन की आवश्यकता है।
सुझाव
- सबसे पहले, स्वास्थ्य सेवाओं की गुणवत्ता सुनिश्चित करना आवश्यक है और सभी हितधारकों की संयुक्त जिम्मेदारी है।
- दूसरे, विनियामक पहलुओं में, बड़े कॉरपोरेट अस्पतालों के लिए जो संभव है, वह छोटे क्लीनिकों और नर्सिंग होम के लिए संभव नहीं हो सकता है, बिना बढ़ी हुई लागत के।
- तीसरे, डॉक्टरों के संघों के प्रतिनिधियों और उन सुविधाओं के प्रकार जिनके लिए विनियमन बनाए जा रहे हैं, साथ ही समुदाय के सदस्यों को ऐसे विनियमन के निर्माण की प्रक्रिया में शामिल किया जाना चाहिए।
- चौथा, राजनीतिक ढीली-ढाली बातें और सनसनीखेज मीडिया की सुर्खियाँ डॉक्टरों और नर्सिंग होम के बारे में आम आदमी के अविश्वास को बढ़ा सकती हैं और स्वास्थ्य सेवा प्रदाताओं के खिलाफ हिंसा में वृद्धि हो सकती है।
- पांचवें और सबसे महत्वपूर्ण बात यह है कि भारत को छोटी स्वास्थ्य देखभाल सुविधाओं और नर्सिंग होम के अलावा एकल डॉक्टर क्लीनिक को बढ़ावा देने की आवश्यकता है।
निष्कर्ष
- भारत की स्वास्थ्य सेवा प्रणाली पहले से ही भर्ती आधारित इन-पेशेंट सेवाओं की ओर झुकी हुई है। इसे ऐसे प्रदाताओं और सुविधाओं को बढ़ावा देने की आवश्यकता है जो कम लागत पर आउट-पेशेंट देखभाल प्रदान करते हैं।
- यह राष्ट्रीय स्वास्थ्य नीति, 2017 के लक्ष्य में योगदान देगा – ऐसी स्वास्थ्य सेवाएँ प्रदान करना जो लोगों पर केंद्रित हों, सुलभ हों, उपलब्ध हों, सस्ती हों और जिनमें गुणवत्ता हो।
भारत में स्वास्थ्य सेवा विनियमन
भारत में स्वास्थ्य सेवा विनियमन में चुनौतियाँ: खंडित विनियामक ढाँचा
- एकीकृत विनियामक ढाँचे की कमी के परिणामस्वरूप अधिकार क्षेत्र में अतिव्यापन और असंगतियाँ होती हैं।
- गुणवत्ता नियंत्रण: सार्वजनिक और निजी स्वास्थ्य सेवा प्रदाताओं के बीच गुणवत्ता मानकों को सुनिश्चित करना एक चुनौती बनी हुई है।
- पहुँच असमानताएँ: ग्रामीण-शहरी विभाजन और सामाजिक-आर्थिक असमानताएँ स्वास्थ्य सेवाओं तक समान पहुँच को प्रभावित करती हैं।
- चिकित्सा शिक्षा: गुणवत्ता मानकों को बनाए रखने के लिए चिकित्सा शिक्षा के विनियमन और स्वास्थ्य सेवा संस्थानों की मान्यता में सुधार की आवश्यकता है।
- भ्रष्टाचार और निगरानी: प्रभावी निगरानी और निगरानी तंत्र की कमी से स्वास्थ्य सेवा क्षेत्र में भ्रष्टाचार और कदाचार को बढ़ावा मिलता है।
आगे की राह
- एकीकृत विनियामक निकाय: स्वास्थ्य सेवा विनियमन को सुव्यवस्थित करने और स्थिरता सुनिश्चित करने के लिए एक एकीकृत विनियामक निकाय की स्थापना करें।
- बढ़ी हुई निगरानी: कदाचार को रोकने और विनियमों के अनुपालन को सुनिश्चित करने के लिए निगरानी और प्रवर्तन तंत्र को मजबूत करें।
- गुणवत्ता का मानकीकरण: देखभाल के एकसमान मानकों को सुनिश्चित करने के लिए स्वास्थ्य सेवा सुविधाओं में मानकीकृत गुणवत्ता नियंत्रण उपायों को लागू करें।
- ग्रामीण स्वास्थ्य सेवा में निवेश: पहुँच संबंधी असमानताओं को दूर करने के लिए ग्रामीण स्वास्थ्य सेवा के बुनियादी ढाँचे और सेवाओं में निवेश बढ़ाएँ।
- क्षमता निर्माण: सेवा वितरण और देखभाल की गुणवत्ता को बढ़ाने के लिए स्वास्थ्य सेवा पेशेवरों के प्रशिक्षण और क्षमता निर्माण में निवेश करें।
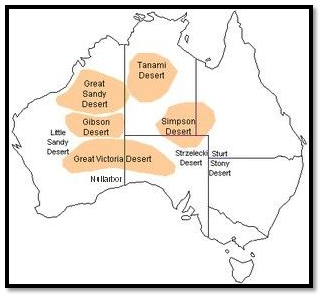
Australia and Oceania [Mapping] / ऑस्ट्रेलिया और ओशिनिया [मानचित्र]
Desert

- Gibson Desert – a central Australian desert
- Great Sandy Desert – a northwestern Australian desert
- Great Victoria Desert – the sixth-largest desert in the world by area, located in south-central Australia.
- Simpson Desert – a central Australian desert
- Little Sandy Desert – a western Australian desert
- Strzelecki Desert – a south-central Australian desert
- Tanami Desert – a northern Australian desert
- Western Desert – a desert located in western Australia, comprising the Gibson, Great Sandy, and Little Sandy deserts.
- Rangipo Desert – a barren light altitude desert on the North Island Volcanic Plateau in New Zealand.
The Central Lowland
- The extensive patch of plain or low land has its existence between the Eastern Highlands and Western Plateau.
- The patch is drained by two rivers such as Murray and Darling which also facilitate the land with irrigation facilities for farming and other essential activities.
- The area is also known as the Great Artesian Basin as it is covered by a number of underground pressurized wells from which the water comes out automatically to the surface. Yet they are not suitable for drinking as they are salty by nature.
The Great Barrier Reef

- This is the largest coral reef in the world.
- It lies along the east coast of Queensland, Australia, in the Pacific Ocean.
- It is about 2,000 kilometers long, in some places, it is as close as 16 kilometers to the coast while in other places it is 200 kilometers away.
- It is one of the natural wonders of the world.
- It is formed by the tiny coral polyps.
The Islands of Australia & Oceania

- The islands situated surrounding the younger most continent in size are collectively known as Oceania. Broadly it has been divided into three major island groups Melanesia, Micronesia, and Polynesia.
- Melanesia is otherwise known as Black Islands and congregated around north and east of Australia. Some of the major islands are East Timor, Fiji, New Caledonia, Papua New Guinea, Solomon Islands, and Vanuatu.
- Micronesia which is also called as Little Islands is the agglomeration of islands such as Guam, Kiribati, Marshall Islands, Federated States of Micronesia, Nauru, Northern Mariana Islands, Palau, and Wake Island.
- Polynesia is otherwise known as Many Lands which expand from islands of Midway in the north to New Zealand in the south and include the series of islands such as the American Samoa Cook Islands, French Polynesia, Niue, Pitcairn, Tokelau, Tonga, Tuvalu, Wallis and Futuna Islands.
- The islands of Oceania have been formed due to the differential activities of volcanoes. The low islands of Micronesia have been formed by building up coral reefs on the rim of the volcanic islands, hence giving it a shape of a Ring which is known as Atolls. The atolls further encircle the lagoons which are characterized by shallow pools of clear water at a very low altitude of just a few feet above sea level.

ऑस्ट्रेलिया और ओशिनिया [मानचित्र]
रेगिस्तान
- गिब्सन रेगिस्तान – एक केंद्रीय ऑस्ट्रेलियाई रेगिस्तान
- ग्रेट सैंडी रेगिस्तान – एक उत्तरपश्चिमी ऑस्ट्रेलियाई रेगिस्तान
- ग्रेट विक्टोरिया रेगिस्तान – क्षेत्रफल के हिसाब से दुनिया का छठा सबसे बड़ा रेगिस्तान, जो दक्षिण-मध्य ऑस्ट्रेलिया में स्थित है।
- सिम्पसन रेगिस्तान – एक केंद्रीय ऑस्ट्रेलियाई रेगिस्तान
- लिटिल सैंडी रेगिस्तान – एक पश्चिमी ऑस्ट्रेलियाई रेगिस्तान
- स्ट्रेज़ेलेकी रेगिस्तान – एक दक्षिण-मध्य ऑस्ट्रेलियाई रेगिस्तान
- तनामी रेगिस्तान – एक उत्तरी ऑस्ट्रेलियाई रेगिस्तान
- पश्चिमी रेगिस्तान – पश्चिमी ऑस्ट्रेलिया में स्थित एक रेगिस्तान, जिसमें गिब्सन, ग्रेट सैंडी और लिटिल सैंडी रेगिस्तान शामिल हैं।
- रंगिपो रेगिस्तान – न्यूज़ीलैंड में उत्तरी द्वीप ज्वालामुखी पठार पर एक बंजर हल्का ऊंचाई वाला रेगिस्तान।
मध्य तराई
- पूर्वी हाइलैंड्स और पश्चिमी पठार के बीच मैदानी या निचली भूमि का विस्तृत क्षेत्र मौजूद है।
- इस क्षेत्र में मरे और डार्लिंग जैसी दो नदियाँ बहती हैं, जो खेती और अन्य आवश्यक गतिविधियों के लिए सिंचाई की सुविधा भी प्रदान करती हैं।
- इस क्षेत्र को ग्रेट आर्टेसियन बेसिन के रूप में भी जाना जाता है क्योंकि यह कई भूमिगत दबाव वाले कुओं से घिरा हुआ है, जहाँ से पानी अपने आप सतह पर आ जाता है। फिर भी वे पीने के लिए उपयुक्त नहीं हैं क्योंकि वे स्वभाव से नमकीन होते हैं।
ग्रेट बैरियर रीफ
- यह दुनिया की सबसे बड़ी कोरल रीफ है।
- यह प्रशांत महासागर में ऑस्ट्रेलिया के क्वींसलैंड के पूर्वी तट पर स्थित है।
- यह लगभग 2,000 किलोमीटर लंबा है, कुछ स्थान इसके तट से 16 किलोमीटर की दूरी पर है जबकि अन्य स्थान 200 किलोमीटर दूर है।
- यह दुनिया के प्राकृतिक अजूबों में से एक है।
- यह छोटे कोरल पॉलीप्स द्वारा निर्मित है।
ऑस्ट्रेलिया और ओशिनिया के द्वीप
- आकार में सबसे युवा महाद्वीप के आसपास स्थित द्वीपों को सामूहिक रूप से ओशिनिया के रूप में जाना जाता है। मोटे तौर पर इसे तीन प्रमुख द्वीप समूहों मेलानेशिया, माइक्रोनेशिया और पोलिनेशिया में विभाजित किया गया है।
- मेलानेशिया को ब्लैक आइलैंड्स के रूप में भी जाना जाता है और यह ऑस्ट्रेलिया के उत्तर और पूर्व में स्थित है। कुछ प्रमुख द्वीप पूर्वी तिमोर, फिजी, न्यू कैलेडोनिया, पापुआ न्यू गिनी, सोलोमन द्वीप और वानुअतु हैं।
- माइक्रोनेशिया जिसे लिटिल आइलैंड्स भी कहा जाता है, गुआम, किरिबाती, मार्शल आइलैंड्स, फेडरेटेड स्टेट्स ऑफ माइक्रोनेशिया, नाउरू, उत्तरी मारियाना द्वीप, पलाऊ और वेक आइलैंड जैसे द्वीपों का समूह है।
- पोलिनेशिया को कई भूमि के रूप में भी जाना जाता है जो उत्तर में मिडवे के द्वीपों से दक्षिण में न्यूजीलैंड तक फैली हुई है और इसमें अमेरिकी समोआ कुक आइलैंड्स, फ्रेंच पोलिनेशिया, नियू, पिटकेर्न, टोकेलाऊ, टोंगा, तुवालु, वालिस और फ़्यूचूना द्वीप जैसे द्वीपों की श्रृंखला शामिल है।
- ओशिनिया के द्वीप ज्वालामुखियों की विभिन्न गतिविधियों के कारण बने हैं। माइक्रोनेशिया के निम्न द्वीप ज्वालामुखी द्वीपों के किनारे पर प्रवाल भित्तियों के निर्माण से बने हैं, जिससे इसे एक वलय का आकार मिला है जिसे एटोल के नाम से जाना जाता है। एटोल लैगून को घेरते हैं, जिसकी विशेषता समुद्र तल से कुछ ही फीट की बहुत कम ऊंचाई पर साफ पानी के उथले तालाब हैं।